Before you complete a profile, please provide the following information about your family. This information is used to help provide appropriate recommendations, about service providers and programs in your community, to your particular family.
You do not have to complete all of the information, and you are welcome to remain anonymous if you like, however some fields are required. Rest assured that any information you provide will only be released to providers that you specifically release it to.
Families are encouraged to create a username and password so that you can return to the system to update your information, learn about new services, and take advantage of the personal success plan.
Welcome!
Using the system is easy! Information you provide is mostly optional, strictly confidential and used only to help match you up with programs and services.
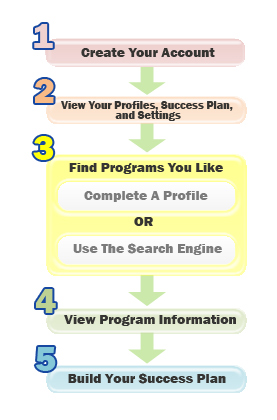
First you will create your account.
Next you will be taken to the "My Profiles, Plan and Settings" page. From there, you can:
Complete a Profile or Search for Programs using the Search Engine.
Completing a Profile lets this system analyze your responses and suggest programs or services that you might not know were available. Profiles are a great way to get started.
"Search For Programs" will help you find specific programs if you already know what types of services you are looking for.
After your Search or Complete A Profile, you may "View Program Information" that may interest you.
If you see one or more programs that look helpful to you, create a Success Plan! Your Plan is a personal list of all the Programs you are interested in. You can edit and print, or add and remove Programs from your Plan any time you wish.